Shoulder MRI: Bursitis, Tendinosis, and Biceps Fluid
Shoulder pain can be real even without a full-thickness rotator cuff tear. Learn what mild MRI findings may mean.

Have your own scan or report? Get a clear, plain-language explanation in minutes.
Why shoulder pain can be significant without a major tear
Many people expect a shoulder MRI to show one clear cause of pain, such as a large rotator cuff tear. But shoulder pain is often more complicated. An MRI may say there is no obvious full-thickness rotator cuff tear, no fracture, and no dislocation, yet still describe findings like mild supraspinatus tendinosis, subacromial-subdeltoid bursitis, or fluid around the long head of the biceps tendon sheath.
These findings can sound minor, but they may still match real pain, stiffness, clicking, weakness, or trouble reaching overhead. This article is general education, not a diagnosis. Your symptoms, physical exam, injury history, and full official MRI report all matter when deciding what a finding means.
A shoulder MRI can look reassuring because there is no major tear, while still showing irritation in the tendons, bursa, or biceps tendon sheath that may contribute to pain.
What the MRI terms mean in plain language
Supraspinatus tendinosis
The supraspinatus is one of the rotator cuff tendons. It helps lift the arm and stabilize the shoulder. Tendinosis means the tendon looks irritated, thickened, or worn on MRI, often from repetitive stress or age-related change. It is different from a full-thickness tear, where a tendon is torn all the way through.
Mild tendinosis or low-grade fraying may be described when the tendon fibers look stressed but not completely torn. This can still hurt, especially with overhead reaching, lifting, throwing, swimming, or sleeping on the affected side.
Subacromial-subdeltoid bursitis
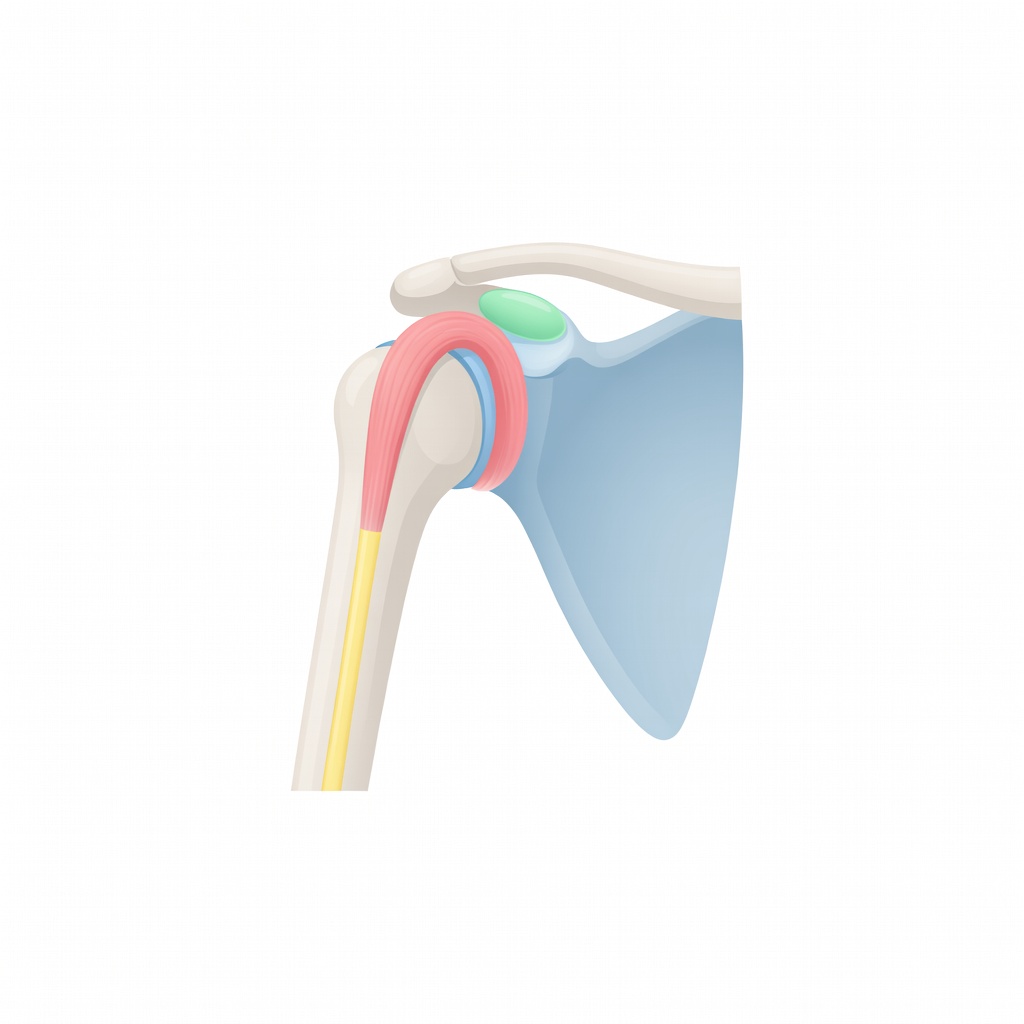
A bursa is a thin, slippery fluid-filled cushion that helps tissues glide smoothly. The subacromial-subdeltoid bursa sits above the rotator cuff and below the acromion and deltoid muscle. When it becomes irritated, the MRI may show a small amount of extra fluid or swelling.
Bursitis can cause pain with reaching out to the side, raising the arm overhead, putting on a jacket, or lying on the shoulder. Sometimes bursitis appears along with rotator cuff irritation or shoulder impingement.
Fluid around the biceps tendon sheath
The long head of the biceps tendon travels through a groove at the front of the shoulder. A small amount of fluid around this tendon may be described as biceps tendon-sheath fluid. In the right clinical setting, this can reflect mild irritation or tenosynovitis, which means inflammation of the tendon lining.
This finding may be more relevant when pain is felt in the front of the shoulder or upper arm, especially with lifting, carrying, reaching, or movements that load the biceps.
No full-thickness tear does not mean nothing is wrong
A full-thickness rotator cuff tear is only one possible source of shoulder pain. The shoulder is a highly mobile joint with many pain-sensitive structures, including tendons, bursae, ligaments, cartilage, labrum, joint lining, and surrounding muscles.
Even mild inflammation or mechanical irritation can be painful because these tissues move repeatedly throughout the day. Small changes may become noticeable when the shoulder is asked to do more than usual, such as during sports, work tasks, home projects, or a new exercise routine.
- Tendinosis can make a tendon less tolerant of load.
- Bursitis can make normal gliding painful.
- Biceps tendon-sheath fluid can suggest irritation at the front of the shoulder.
- Impingement can pinch or rub tissues during overhead motion.
- Partial-thickness injury may be subtle and harder to see than a complete tear.
Common reasons these MRI findings happen
Mild shoulder MRI findings often develop from a combination of mechanics, activity, and tissue sensitivity rather than one single event. Common contributing factors include:
- Overuse: Repeated lifting, reaching, pushing, pulling, or overhead work can irritate the rotator cuff and bursa.
- Sports activity: Throwing sports, swimming, tennis, volleyball, weight training, and climbing can load the shoulder repeatedly.
- Shoulder impingement: Some people have pain when the rotator cuff and bursa are compressed during arm elevation.
- Age-related tendon change: Tendons can become less smooth and more prone to irritation over time, even without a major injury.
- Posture and muscle control: Shoulder blade position and rotator cuff strength can affect how smoothly the joint moves.
- Recent strain or minor trauma: A pull, fall, or awkward lift may flare a tendon or bursa without causing a complete tear.
What a full shoulder MRI report usually covers
A complete diagnostic shoulder MRI is reviewed in multiple planes and sequences. That means the radiologist looks at the shoulder from different angles and with different MRI settings, not just one slice or one series. This is important because some findings are only visible on certain views.
A full shoulder MRI report may comment on:
- Bones and alignment: Whether there is fracture, bone bruising, arthritis, dislocation, or abnormal bone shape.
- Rotator cuff tendons: The supraspinatus, infraspinatus, subscapularis, and teres minor are checked for tendinosis, partial tear, full-thickness tear, or retraction.
- Rotator cuff muscles: The report may mention muscle bulk, fatty atrophy, or swelling.
- Biceps tendon: The radiologist may assess position in the groove, tearing, tendinosis, and fluid in the tendon sheath.
- Labrum: The labrum is a rim of cartilage around the socket. Tears can be difficult to assess and may require careful review.
- Cartilage and joint space: The report may describe arthritis, cartilage thinning, or joint fluid.
- Bursa: Extra fluid in the subacromial-subdeltoid bursa may suggest bursitis.
- AC joint: The acromioclavicular joint at the top of the shoulder can show arthritis or irritation that contributes to pain.
Sometimes a report or image review is described as limited because only one MRI series is available, or the full set of images is not being reviewed. In that situation, subtle tendon, labrum, cartilage, or ligament findings may not be fully assessed. The official radiology report from the complete exam is the most important imaging document to review with a clinician.
How doctors connect MRI findings with symptoms
MRI findings do not always perfectly match pain. Some people have mild findings and significant symptoms. Others have visible tendon changes but little pain. That is why clinicians usually combine the MRI with a physical exam and history.
Important clinical clues may include where the pain is located, whether there was an injury, which movements hurt, whether there is weakness, and whether the shoulder feels unstable. For example, front-of-shoulder pain may raise attention to the biceps tendon, while pain with overhead motion may fit with bursitis, tendinosis, or impingement patterns.
Treatment options vary depending on the person and the diagnosis. In many non-emergency situations, clinicians may discuss activity modification, physical therapy, anti-inflammatory strategies when appropriate, injections, or specialist referral. Surgery is not automatically needed just because an MRI mentions tendinosis, bursitis, or biceps sheath fluid.
Key takeaways
- An MRI can show no full-thickness rotator cuff tear but still reveal painful irritation.
- Mild supraspinatus tendinosis means the tendon appears stressed or worn, not completely torn.
- Bursal fluid can reflect bursitis, which may hurt with overhead reaching or lying on the shoulder.
- Fluid around the biceps tendon sheath may relate to front-of-shoulder pain in the right setting.
- A complete MRI report is more reliable than a single image series or limited review.
- Imaging results should be interpreted together with symptoms and a physical exam.
When to talk to your doctor
Talk to your doctor, orthopedist, sports medicine clinician, or physical therapist if shoulder pain is persistent, limits daily activities, interferes with sleep, or is associated with weakness or reduced range of motion. Seek prompt medical care for severe pain after trauma, new deformity, inability to lift the arm, numbness, fever, or rapidly worsening symptoms.
Remember: this article is for general education and is not a diagnosis or a substitute for your official MRI report and medical evaluation.
Get AI-powered analysis of your CT or MRI scan
Upload your DICOM files and receive a clear, patient-friendly report in minutes.
Analyze my scan