Osgood-Schlatter on MRI: Teen Knee Pain Explained
MRI words like marrow edema and fragmentation can sound scary. Learn how Osgood-Schlatter disease causes pain below the kneecap.

Have your own scan or report? Get a clear, plain-language explanation in minutes.
Why an MRI report can sound alarming
If your teen has pain at the bump just below the kneecap, an MRI report may use words like marrow edema, fragmentation, apophysitis, or patellar tendon insertional change. Those terms can sound serious. In many growing athletes, however, this pattern points to a common growth-related overuse condition called Osgood-Schlatter disease.
This article is general education and not a diagnosis. A clinician who knows the symptoms, exam findings, sport activities, and full imaging study is the right person to explain what the MRI means for a specific child.
What is Osgood-Schlatter disease?
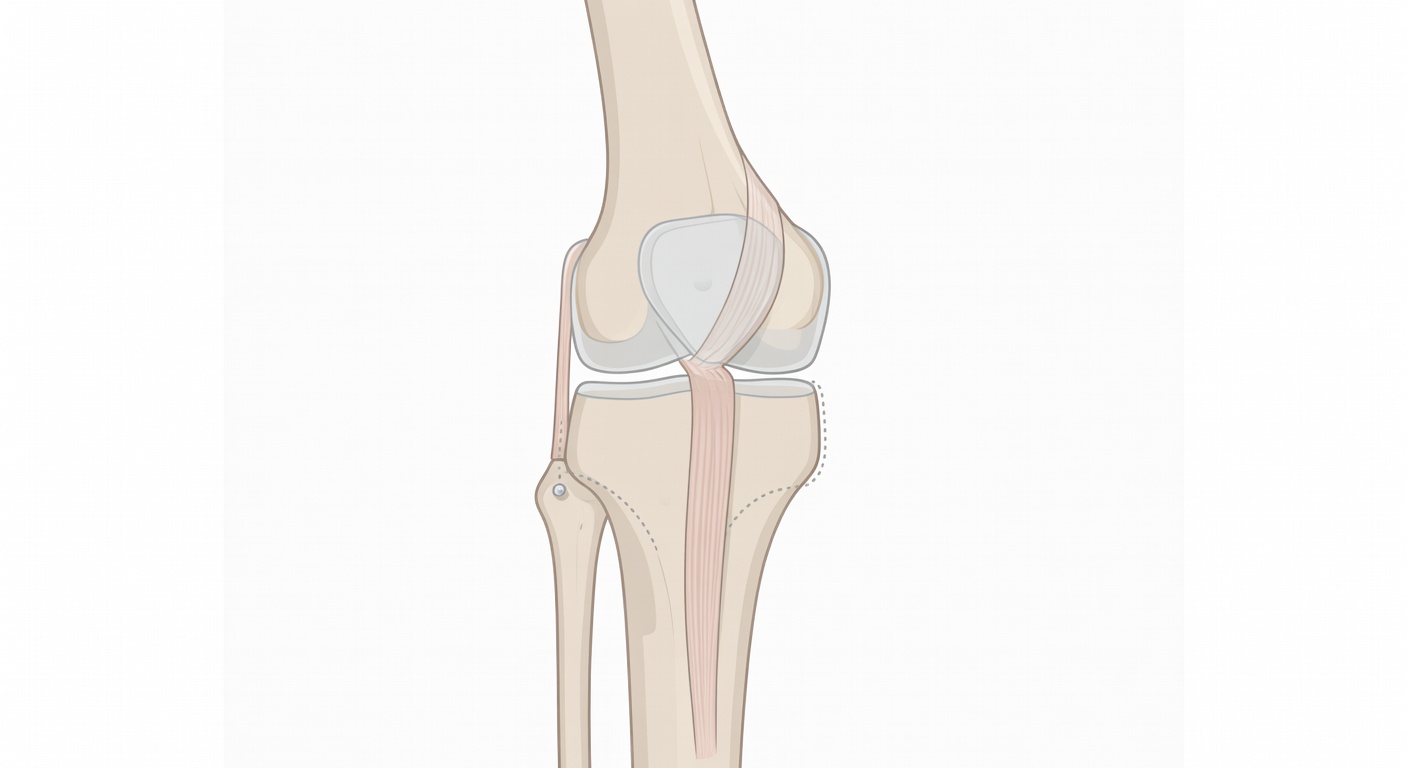
Osgood-Schlatter disease is irritation where the kneecap tendon, called the patellar tendon, attaches to the upper shinbone. That attachment point is the tibial tubercle, the bony bump you can feel a few centimeters below the kneecap.
In children and teens, this area is not fully mature bone yet. It includes a growth region called an apophysis. An apophysis is a growth center where a tendon pulls on bone. During growth spurts, sports that involve running, jumping, sprinting, squatting, or kicking can repeatedly tug on this area. Over time, that traction can make the tibial tubercle sore and swollen.
In plain language: the tendon is repeatedly pulling on a growing bone attachment, and the irritated growth area becomes painful.
Why the pain is felt at the bump below the kneecap
The pain of Osgood-Schlatter disease is usually felt directly over the tibial tubercle. This is because that is where the patellar tendon anchors into the shinbone. When the quadriceps muscle on the front of the thigh tightens, it pulls on the kneecap and patellar tendon. That force travels to the tibial tubercle.
Teens may notice pain with:
- Running, especially sprinting or hills
- Jumping and landing
- Stairs
- Squats or lunges
- Kneeling directly on the bump
- Sports such as basketball, soccer, volleyball, football, gymnastics, and track
The bump can look prominent, feel tender, or be sore after activity. In some teens, both knees are involved, though one side may hurt more.
What MRI may show in Osgood-Schlatter disease
MRI is very sensitive to fluid and inflammation-like changes. In Osgood-Schlatter disease, a knee MRI may show a classic pattern centered at the tibial tubercle. Common report phrases include:
- Marrow edema-like signal: increased fluid-sensitive signal in the bone near the tibial tubercle, reflecting stress or irritation.
- Fragmented or prominent tibial tubercle apophysis: an uneven-looking growth area where the tendon attaches. This can be part of the Osgood-Schlatter spectrum in a growing knee.
- Soft-tissue edema: mild swelling in the tissues in front of the upper shinbone.
- Distal patellar tendon signal or thickening: mild irritation where the patellar tendon inserts on the tibial tubercle.
- Trace or small joint effusion: a small amount of extra knee fluid, which can happen with irritation or injury.
These findings matter most when they match the teen's pain location and activity history. For example, tibial tubercle edema on MRI is more meaningful if the child is tender right at the bump below the kneecap and has pain during jumping or running.
How this differs from a fracture
Parents often worry that words like fragmentation or edema mean a broken bone. Sometimes an acute injury can affect the tibial tubercle, but Osgood-Schlatter disease is usually a traction-related overuse process rather than a displaced fracture.
On MRI, a more concerning acute fracture pattern may show a clear break line, displacement of a bone fragment, major swelling, or a history of a sudden painful event. In contrast, Osgood-Schlatter-type change is typically centered at the tendon attachment and growth area, often with an intact patellar tendon and no obvious displaced fragment.
That said, imaging language should always be interpreted with the whole story. A sudden pop, inability to straighten the knee, inability to bear weight, or major swelling after a specific injury deserves prompt medical evaluation.
How this differs from an ACL, PCL, or meniscus injury
Osgood-Schlatter pain is usually very local: the sore spot is the bump below the kneecap. Ligament and meniscus injuries often cause different symptoms.
- ACL injury: often follows a twisting or pivoting event, sometimes with a pop and rapid swelling.
- PCL injury: may occur after a blow to the front of the shin or a fall onto a bent knee.
- Meniscus tear: may cause joint-line pain, catching, locking, or pain with twisting.
- Osgood-Schlatter disease: usually causes tenderness at the tibial tubercle and pain with running, jumping, kneeling, or stairs.
MRI reports may state that the ACL, PCL, collateral ligaments, and menisci appear intact, especially when no definite tear is seen. Sometimes a report also notes that a single MRI series cannot fully assess every structure, because radiologists use multiple views together to make the final interpretation.
Why activity modification is often discussed
Osgood-Schlatter disease is related to repeated traction. That is why clinicians often discuss activity modification rather than complete rest forever. The goal is usually to reduce the activities that strongly flare pain while maintaining safe movement and fitness when possible.
Activity modification may include reducing jumping volume, taking breaks from painful drills, changing practice intensity, or temporarily avoiding kneeling and deep squats. A clinician may also discuss stretching, strengthening, ice after activity, or physical therapy focused on the quadriceps, hamstrings, hips, and movement mechanics.
The key idea is that pain is a signal. Pushing through significant pain at the tibial tubercle can keep the growth area irritated. On the other hand, many teens can stay active in some form when symptoms are monitored and activities are adjusted under appropriate guidance.
What if the MRI finds more than one thing?
Knee MRIs can reveal more than one finding. For example, a report may describe Osgood-Schlatter-type changes and also mention a discoid lateral meniscus. A discoid meniscus is a shape variant where the outer meniscus is broader than usual. It is present from development, not caused by a recent workout.
A discoid meniscus may be silent, or it may contribute to symptoms such as popping, snapping, pain on the outer side of the knee, or locking if it becomes unstable or torn. If an MRI says there is a likely discoid lateral meniscus but no definite tear, the clinician will usually compare that finding with the teen's symptoms. Pain at the tibial tubercle points more toward Osgood-Schlatter disease, while locking or outer joint-line symptoms may raise different questions.
Helpful questions to ask about the MRI
If the report feels confusing, it can help to ask focused questions at the follow-up visit:
- Do the MRI findings match the exact spot where my teen has pain?
- Is the patellar tendon intact?
- Is there any displaced fracture or avulsion injury?
- Do the ACL, PCL, collateral ligaments, and menisci look intact on the full study?
- Is the discoid meniscus, if present, likely related to the symptoms?
- What activities should be reduced, and what activities are okay for now?
- What signs would mean the knee needs re-checking sooner?
When to talk to your doctor
Talk to a doctor or qualified clinician if a teen has ongoing knee pain, swelling, limping, pain that limits sports or daily activities, or tenderness at the bump below the kneecap. Seek urgent care if there is a sudden injury with a pop, major swelling, visible deformity, inability to bear weight, fever, redness, severe night pain, or inability to straighten the knee. This information is for general education only and should not be used as a diagnosis or a personal treatment plan.
Get AI-powered analysis of your CT or MRI scan
Upload your DICOM files and receive a clear, patient-friendly report in minutes.
Analyze my scan