Rotator Cuff Tendinopathy and Shoulder Bursitis on MRI
Learn what shoulder MRI terms like tendinopathy, bursitis, partial tear, AC arthritis, and impingement may mean.

Have your own scan or report? Get a clear, plain-language explanation in minutes.
Why shoulder MRI reports can sound worrying
Shoulder MRI reports often use technical words such as rotator cuff tendinopathy, subacromial-subdeltoid bursitis, partial-thickness tear, AC joint arthritis, or impingement. These terms can sound alarming, especially when shoulder pain makes it hard to lift the arm, sleep comfortably, or reach overhead.
In many MRI reports, the key message is not a large full-thickness tendon tear, but rather a pattern of tendon irritation, mild fraying, possible small partial tearing, joint wear, and fluid in a nearby bursa. This article explains what those findings commonly mean in plain language. It is general education, not a diagnosis, and it cannot replace a review of your full MRI and physical exam by a medical professional.
The rotator cuff: the shoulder’s stabilizing tendon group
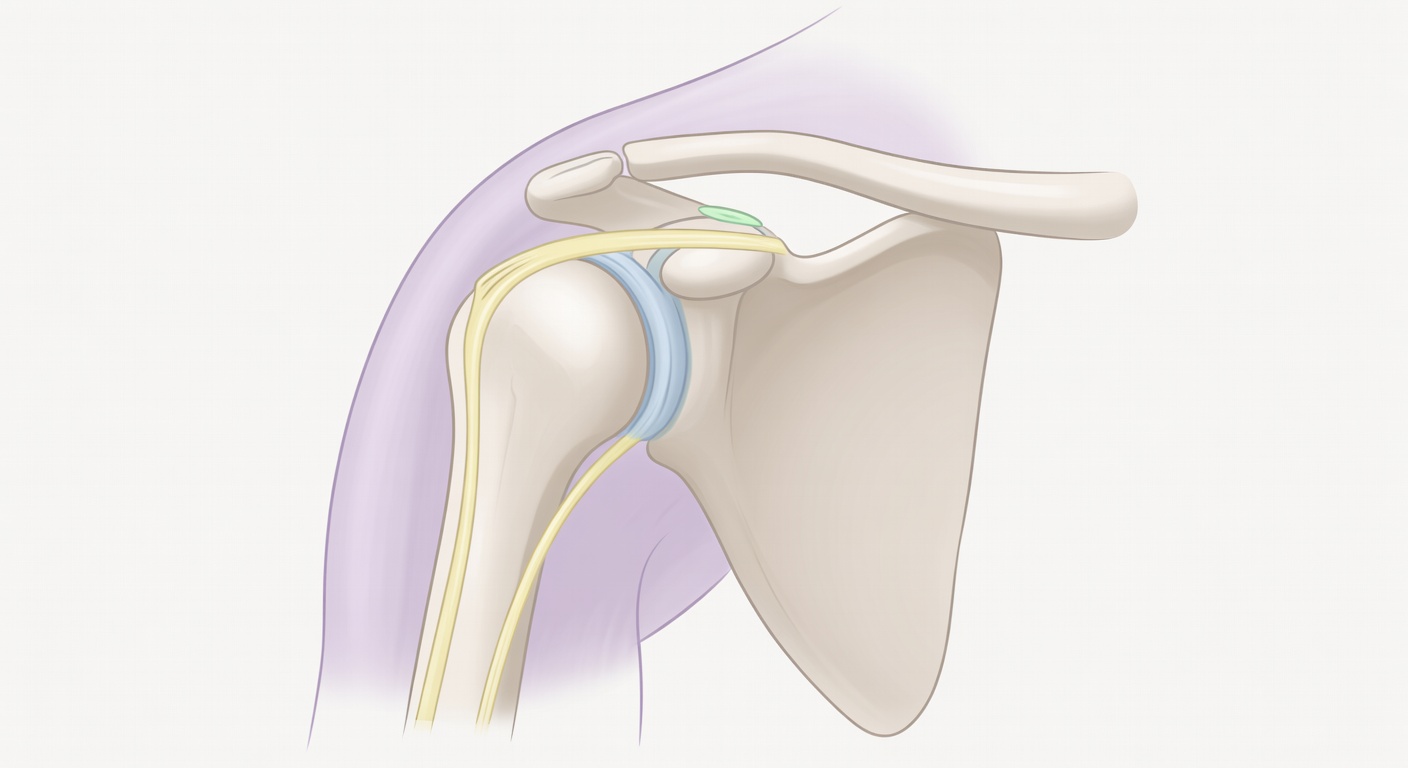
The rotator cuff is a group of muscles and tendons that helps lift and rotate the arm while keeping the ball of the upper arm bone centered in the shoulder socket. The tendon most often mentioned on MRI is the supraspinatus tendon, which runs under the bony roof of the shoulder, called the acromion.
Because this area is narrow and moves a lot, the rotator cuff can become irritated over time or after a change in activity. Pain may be felt on the outside of the upper arm, the front of the shoulder, or deep in the shoulder. It may worsen with reaching overhead, lifting away from the body, putting on a jacket, or lying on the affected side.
What is rotator cuff tendinopathy?
Tendinopathy means the tendon looks irritated, overloaded, thickened, or mildly worn on imaging. On MRI, this may appear as increased signal or uneven texture within the tendon. It does not necessarily mean the tendon is completely torn.
Common report phrases include:
- Mild supraspinatus tendinopathy: irritation or wear in one of the main rotator cuff tendons.
- Insertional tendinopathy: changes near where the tendon attaches to the upper arm bone.
- Footprint changes: changes at the tendon’s attachment site.
- Enthesopathic change: stress-related or degenerative change where tendon meets bone.
Tendinopathy is usually interpreted alongside symptoms. Some people have tendon changes on MRI with little pain, while others have significant pain even when imaging changes are described as mild.
Partial tear versus full-thickness tear
MRI reports may mention a possible small partial tear or state that a partial tear cannot be excluded. A partial-thickness tear means some tendon fibers are damaged, but the tendon is not torn all the way through. A full-thickness tear means the tear extends through the entire tendon thickness. A large full-thickness tear may be associated with tendon retraction, meaning the tendon has pulled back from its attachment.
Many reports specifically say there is no definite full-thickness rotator cuff tear or no tendon retraction. That distinction matters because treatment planning is different for a mild tendinopathy or small partial tear than for a large complete tear with major weakness.
An MRI finding is one piece of the puzzle. Strength, range of motion, pain pattern, injury history, and daily function all help determine what the finding means.
What is subacromial-subdeltoid bursitis?
A bursa is a thin, slippery fluid-filled sac that helps tissues glide smoothly. The subacromial-subdeltoid bursa sits above the rotator cuff and below the acromion and deltoid muscle. When it becomes irritated, MRI may show extra fluid or swelling in this space.
Bursitis means inflammation or irritation of the bursa. It can occur along with rotator cuff tendinopathy because the tendon and bursa share the same tight space under the shoulder roof. When the arm is lifted, irritated tissue can be compressed or pinched, which may cause a painful arc of motion.
Why overhead movement hurts
Overhead motion narrows the space between the upper arm bone and the acromion. If the rotator cuff tendon is irritated, the bursa is inflamed, or the AC joint has bony changes, that space may feel crowded. This is one reason MRI reports may use the term impingement or subacromial impingement configuration.
Impingement is not just an MRI diagnosis. It describes a pattern where tissues under the shoulder roof become painful during certain movements. Posture, shoulder blade control, rotator cuff strength, stiffness, activity load, and anatomy can all contribute.
How AC joint arthritis fits in
The AC joint, or acromioclavicular joint, is the small joint on top of the shoulder where the collarbone meets the acromion. MRI reports may describe AC joint arthritis, degenerative change, or bone spurs. These are wear-related changes that may or may not be painful.
AC joint changes can sometimes contribute to narrowing under the acromion. They can also cause pain directly on top of the shoulder, especially with cross-body reaching, push-ups, bench press, or carrying heavy bags. A clinician may press on the AC joint or perform specific movement tests to see whether it matches the pain.
Why one MRI sequence may not tell the whole story
A complete shoulder MRI usually includes multiple views and sequence types. Some sequences show fluid and inflammation well. Others show anatomy, bone marrow, muscle, and tendon structure. If only one series or a limited set of images is reviewed, the report may say that the exam is limited or that small tears, labral injuries, cartilage problems, or biceps tendon issues cannot be fully excluded.
This is why the official radiology report and the full image set are important. A single MRI slice or one sequence may suggest bursitis or tendinopathy, but final interpretation should use all available images plus the clinical exam.
How doctors connect MRI findings with the exam
Shoulder pain is usually assessed with both imaging and hands-on examination. A clinician may check:
- Range of motion: how far the arm can move actively and passively.
- Strength: whether the rotator cuff can resist pressure in different positions.
- Pain location: front, side, top, or deep inside the shoulder.
- Impingement signs: whether certain movements reproduce the familiar pain.
- Neck and nerve symptoms: because neck problems can sometimes mimic shoulder pain.
For example, mild tendinopathy on MRI with normal strength may be approached differently than similar imaging with sudden weakness after an injury. The same MRI words can have different meaning depending on the person’s story and exam.
What physical therapy often focuses on
For rotator cuff tendinopathy and mild bursitis, care often starts with non-surgical approaches. Physical therapy commonly focuses on improving how the shoulder moves, reducing painful overload, and building strength gradually.
Therapy may include:
- Activity modification: reducing or changing painful overhead lifting while symptoms calm down.
- Shoulder blade mechanics: improving how the scapula moves during reaching.
- Rotator cuff strengthening: starting with controlled, low-irritation exercises and progressing over time.
- Mobility work: addressing stiffness in the shoulder capsule, chest, or upper back.
- Load management: returning to work, sport, or gym activity in a planned way.
Some people also discuss anti-inflammatory medicines, heat or ice, or injections with a clinician. These choices depend on medical history, symptom severity, exam findings, and personal goals.
When to talk to your doctor
Talk with a doctor, orthopedist, sports medicine clinician, or physical therapist if shoulder pain is not improving, limits daily activities, or keeps you from sleeping. Seek prompt medical care after a fall or injury, or if you develop sudden major weakness, numbness, fever, severe swelling, or rapidly worsening pain.
Bring your full MRI report, not just a single image or summary. Ask how the imaging findings match your strength, range of motion, and pain pattern. This article is for general education only and is not a diagnosis or personal medical advice.
Get AI-powered analysis of your CT or MRI scan
Upload your DICOM files and receive a clear, patient-friendly report in minutes.
Analyze my scan